
Human Errors in Drug Manufacturing
- Binh Nguyen
- Aug 1, 2025
- 2 min read

How many of you use "human errors" as a reason of root cause in your conclusion of an investigation?
A. Per Human error - Wikipedia: it is an action that has been done but that was "not intended by the actor; not desired by a set of rules or an external observer; or that led the task or system outside its acceptable limits.
B. Here are some types of human errors: Procedural, Omission, Calculation Mistakes, Communication Errors, Misinterpretation, Improper Execution, Data Management Issues
Failure to Follow Instructions, Task Confusion, and Monitoring Failures.
LET ME TAKE YOU THROUGH SOME EXAMPLES AND CRITICAL THINKING OF PREVENING HUMAN ERRORS
C. Because we are humans, errors do occur. Here are some regulatory and scientific questions and answers:
Is it ok to write "human error" as a root cause in the investigation conclusion?
This really depends on what the situation is. For example,
a. If the human error truly happened (i.e. calculation error or accidentally spill a weight unit), then describe as such and this may be deemed to be acceptable provided that you can minimize repeat of such human error
b. If no root cause was found (i.e. particulate in vials) and "human error" is the blame, this may not be ok especially if it you "consistently" use this reason (i.e. the "human error" blame is used more than once especially for a similar event)
How do we minimize or prevent human errors from occurring?
Continue with the scenarios above
a. Calculation error: create a validated calculation platform
Accidentally spill a weight unit: discuss issue with operator and come up with probable solutions to minimize this error and incorporate into training
b. Particulate matter: this is a serious issue that demands proper root cause assessments - blaming on "human error" can lead to serious regulatory action especially if products with PM are found in retain samples and the market
In both scenarios a and b, the key is to design a quality system to minimize risk. Particularly in b scenario, evaluate
materials: are you introducing PM during container/closures, API, and excipients? If so, how do you reduce this?
facilities/equipment: are facilities and equipment designed and cleaned to prevent/minimize PM?
production: is workflow design adequate to prevent/minimize PM? are people gowned adequately to work in clean room environment? Is the visual inspection robust to catch PM?
lab: is QC monitoring adequate to catch PM? What measures can QC testing be added to help detect PM?
THE BOTTOM LINE MESSAGE: MINIMIZE RISKS wherever and whenever you can
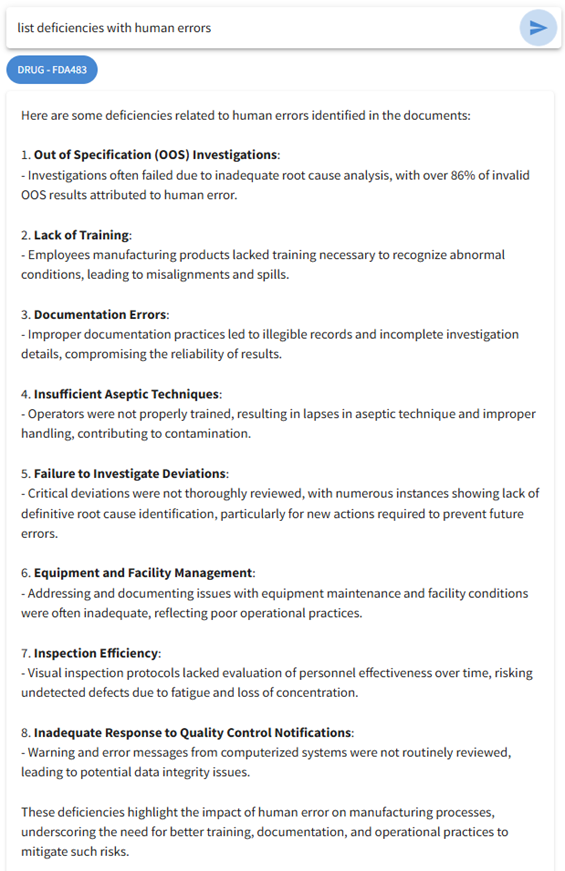
Here are some answers given by ieQip AI based on FDA-483 database so companies can learn from historical mistakes of others. Each one of these deficiencies is associated with an FDA-483...




Comments